

The Irish healthcare system and UHC - Q&A
How is the Irish system financed?
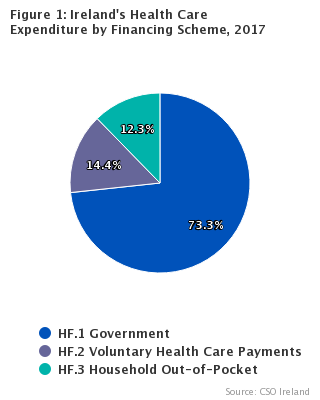
The Irish health system is largely financed through three means:
General taxation = 73%: Most of the health services are paid through general taxation.
Private insurance = 15%: Even though 45% of the population have voluntary health insurance, this contributes 15% to overall health financing. Most of this expenditure relates to care in private secondary care facilities.
Out of pocket charges = 12%: Unusually in a high-income European country, Ireland is the only Western European country that does not offer universal coverage of GP and primary care, with 60% of the population paying out of pocket for GP care and up to €80 per month for drugs as well as paying for other primary care services.

(Image created by Dr Eoin Kelleher)
What does the two-tier system mean?
Roughly one third of the population can receive a ‘medical card’ on the basis of a means threshold assessment. This provides primary care and public hospital services without charge.
However, there can be long waiting times to see hospital consultants in public hospitals, impacting diagnosis and treatment.
Accessing hospital services is often referred to as ‘two-tier’, as those who can afford to pay for private hospital care and/ or have voluntary health insurance can gain quicker access to diagnosis and treatment, even in the public hospital system.
But in reality, there are ‘multiple tiers’ in the Irish healthcare system.
Arguably the most vulnerable group of the population are those who cannot afford voluntary insurance, but who are just above the threshold to receive a medical card, facing the prospect of charges to access primary care and lengthy delays if they require secondary care.
What would universal healthcare look like in terms of primary care?
Only patients with a medical card or doctor visit card (~45% of adults) can access GP-care for free, purchase prescription-medications through a small prescription charge and access primary care services for free.
All other patients have to pay for primary care and GP services, and medications up to €80 per month.
Ireland is the only country in Western Europe without universal coverage of GP and primary care. Many patients struggle to pay to see a GP and pay for medications.
This mixture of pubic-private care has led to Ireland having a mal-funded, badly-integrated primary care service.
We can have universal primary healthcare if it is planned and resourced, with the involvement of GPs and primary care staff. Increasing access to GP-visit cards and Medical Cards, would enable more of the population engage with GP and primary care services. It would deliver enhanced resourcing for General Practice for GP teams.

‘63 per cent of private patients delayed going to see a GP due to cost, while 68 per cent delayed seeing a consultant for this reason’
What is Sláintecare?
In June 2016, the Committee on the Future of Healthcare was established (see here) as part of the 2016 Programme for Government.
Deputy Roisin Shortall was elected chairperson, there was a call for public submissions and the Committee held 30 public hearings and published two interim reports.
The ‘Report of the Committee on the Future of Health, Sláintecare Report’ was published on 30th May 2017. Every political party signed up to Sláintecare and the government cabinet was agreed that the Minister for Health would establish an implementation office in the health department, appoint a lead to the office and produce a draft implementation plan by December 2017.
The main aim of Sláintecare is to provide universal access to timely, quality integrated care for everyone in Ireland.
Sláintecare had five main sections and appendices analysing the submissions received and costing the entitlement expansion.
The five sections in Sláintecare addressed:
1. Population health profile: To enable strong population health approaches support individual’s health, address the social determinants of health and reduce health inequalities.
2. Entitlements and access to healthcare: The report recommended a clear entitlement to universal healthcare, underpinned by legislation, involving a significant expansion of care to meet population health needs, as well as the disentanglement of private care from public hospitals.
3. Integrated care: Centred on reorienting the system towards primary and community care.
4. Funding: Recommending the establishment of a single National Health Fund, which would combine general taxation revenues as well as some earmarked taxes and levies. Over time an increased proportion of the overall health budget would come from public, pooled resources and less from private payments.
5. Implementation

Doctors Alliance for Better Public Healthcare
A group of medical professionals in Ireland set up Doctors Alliance for Better Public Healthcare in 2007. Their aim was to:
Advocate for the requirement to develop publicly-funded healthcare- rather than let the market supply poorly coordinated private services.
Highlight that public services, including hospitals and GP services, are under-funded.
Articulate that the National Treatment Purchase Fund (NTPF) would not support the reduction in hospital waiting lists.
Show that the Irish system needed more hospital beds.
More consultants and GPs would be needed-through agreement of new contracts.
Their submission can be gound here:
One of their presentations can be found below:
What was the Univeral Health Insurance model, which was promised in 2011?
The 2011 Programme for Government promised the delivery of universal healthcare, through a system of Universal Healthcare Insurance (UHI), by 2019.
On 2nd April 2014, Minister James Reilly published “The Path to Universal Healthcare: White Paper on Universal Health Insurance” and stated that the system would not cost more money. The ‘Dutch’ model of financing healthcare, in a UHI system, had by 2014 seen its expenditure soar and services rationed.
The system of UHI envisaged multiple competing insurance companies interacting with multiple competing providers, with citizens eligible to a basket of healthcare services.
However, costings by the ESRI showed that the model of UHI, as proposed would be between €0.6b- €2b more per annum, and the government would continue to fund 70% of the system and out of pocket charges would persist (average €379 per annum).
The subsequent Minister for Health Leo Varadkar went on say in 2015 that UHI, proposed by his predecessor James Reilly, was ‘not affordable, now or ever’.
Dr Sara Burke subsequently stated, ‘the universal health insurance model adopted by this Government was the wrong one. But its intention of universal healthcare was right.’
‘Private’ patients treated within our public hospitals: What is the De Buitléir Report?
One of the key platforms of Sláintecare was removing private healthcare from public hospitals.
Currently patients with voluntary insurance can bring income, outside of taxation, to our public hospitals. It can also bring income to consultants working in public hospitals.
Inequity within our public hospitals has been highlighted for years and was mentioned in an OECD Report in 2017.
The DeBuitléir Report in 2019 set about costing the loss in revenue for public hospitals, if private income was removed.
It estimated that €626 million extra, per annum, would ultimately be needed to replace this lost income nationally, for our public hospitals.
It was stated at the time that: ‘The De Buitléir report published on Monday sends a clear message to government – that the removal of private work from public hospitals can and should happen. It states that “the Government should send a clear signal through legislation that, from a specific date in the future, no private activity in public hospitals will be permitted‘.

Image by Dr Eoin Kelleher
What does the World Health Organisation say about UHC?
The WHO recommends that all countries, like Ireland, should implement Universal Healthcare for their population.
Universal health coverage means that all people have access to the health services they need, when and where they need them, without financial hardship.
Universal healthcare includes the full range of essential health services, from health promotion to prevention, treatment, rehabilitation, and palliative care.